Veterans Health Care: Training and Improved Oversight Needed for Reviewing and Reporting Providers with Clinical Care Concerns
Fast Facts
The Department of Veterans Affairs requires its medical facility officials to review a provider's care when safety concerns are raised. If VA facility officials decide a provider should no longer provide care to veterans, they report their determination to a national database and the states where the provider is licensed.
However, at the 5 VA medical facilities we analyzed, we found that some reviews exceeded suggested timeframes or were missing required documentation. We also found that VA officials didn't report 7 providers who should have been reported, putting patient safety at risk.
Our recommendations address these issues.

Person in white coat with stethoscope around their neck.
Highlights
What GAO Found
Veterans Health Administration (VHA) medical facility officials are responsible for reviewing the clinical care delivered by their providers when concerns arise. GAO identified 104 providers with clinical care concerns (such as practicing in a manner that is unsafe or inconsistent with industry standards of care) at five selected VHA medical facilities between January 2020 and July 2024. GAO found these facilities did not consistently adhere to VHA policy when conducting quality reviews, or reporting providers to state licensing boards or the National Practitioner Data Bank. All five facilities also had missing or incomplete review documentation. As of March 2026, VHA has developed some mandatory training for facility staff related to credentialing providers, but not any on quality review and reporting processes. By failing to follow VHA policy, facilities increase the risk that these processes are conducted incorrectly and that these providers may continue to provide unsafe care to veterans.
State Licensing Board Reporting Process for VHA Providers, as of July 2024
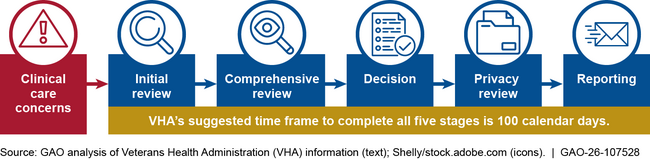
Related to reporting, GAO also found these five facilities did not initiate processes to determine whether seven providers should have been reported to state licensing boards or the National Practitioner Data Bank. Completing the review process for these providers will provide VHA assurance that any identified quality concerns will be properly assessed and that the providers who should be reported are reported. Timely reporting helps reduce the risk that other VHA facilities or community hospitals and clinics hire providers with unreported clinical care issues, thereby potentially putting patients at risk.
In addition, GAO found that VHA oversight of review and reporting processes at medical facilities was limited in ensuring adherence to VHA policy requirements. Specifically, VHA’s oversight methods—which include a tracking tool and an annual facility self-assessment and audit—are not designed to assess adherence with all timeliness and documentation requirements. These limitations prevent VHA from comprehensively and consistently overseeing processes for monitoring provider clinical performance and ensuring safe, quality health care for veterans.
Why GAO Did This Study
VHA is responsible for ensuring providers deliver safe care to veterans at its more than 170 medical facilities. However, VHA has faced challenges ensuring providers with clinical care concerns undergo timely and documented reviews, and are reported to external entities when appropriate.
GAO was asked to examine VHA processes for reviewing concerns about providers’ clinical care. This report assesses (1) selected VHA medical facilities’ adherence to VHA policies for reviewing and reporting providers with clinical care concerns; and (2) VHA’s oversight of quality review and reporting processes for providers with clinical care concerns.
GAO reviewed VHA policy documents and interviewed VHA officials. GAO also selected a non-generalizable sample of five VHA medical facilities (based on factors such as facility complexity) and identified providers with clinical care concerns from January 2020 through July 2024. This time frame included the most recent facility meeting minutes and allowed for reviews and reporting to be completed. For each provider, GAO reviewed available documentation and interviewed local and regional VHA officials.
Recommendations
GAO is making seven recommendations to VHA, including developing training, completing the reporting process for certain providers, and ensuring that oversight methods assess compliance with VHA’s review and documentation requirements. VA concurred or concurred in principle with GAO’s seven recommendations and identified steps it plans to take.
Recommendations for Executive Action
| Agency Affected | Recommendation | Status |
|---|---|---|
| Veterans Health Administration | The Under Secretary for Health should develop training materials related to quality reviews, the NPDB adverse privileging process, and the SLB reporting process. As appropriate, these trainings should include reporting requirements; documentation requirements and preferred storage location; time frames; and provider scenarios. The trainings should be required for relevant VHA medical facility staff. (Recommendation 1) |
When we confirm what actions the agency has taken in response to this recommendation, we will provide updated information.
|
| Veterans Health Administration | The Under Secretary for Health should initiate the SLB or NPDB reporting process for the seven providers we identified to determine if SLB or NPDB reporting is warranted for those providers. (Recommendation 2) |
When we confirm what actions the agency has taken in response to this recommendation, we will provide updated information.
|
| Veterans Health Administration | The Under Secretary for Health should (1) assess the extent to which VHA medical facilities are meeting the suggested time frame in VHA policy when conducting external reviews, such as focused clinical care reviews; (2) assess the risk exceeding the suggested time frame poses to addressing clinical care concerns and to patient care; and (3) make changes to address identified risks as appropriate. (Recommendation 3) |
When we confirm what actions the agency has taken in response to this recommendation, we will provide updated information.
|
| Veterans Health Administration | The Under Secretary for Health should (1) assess the extent to which VHA medical facilities are meeting the suggested time frame in VHA policy when conducting the SLB reporting process; (2) assess the risk exceeding the suggested time frame poses to reporting substantiated clinical care concerns and to patient care; and (3) make changes to address identified risks as appropriate. (Recommendation 4) |
When we confirm what actions the agency has taken in response to this recommendation, we will provide updated information.
|
| Veterans Health Administration | The Under Secretary for Health should review and clarify its policy requirements as to when to begin the SLB reporting process when a clinical care concern is identified. (Recommendation 5) |
When we confirm what actions the agency has taken in response to this recommendation, we will provide updated information.
|
| Veterans Health Administration | The Under Secretary for Health should ensure that the facility tracking tool for reviewing and reporting providers with clinical care concerns be updated to include confirmation that required quality review and reporting documentation is complete and saved in the appropriate location at the facilities. (Recommendation 6) |
When we confirm what actions the agency has taken in response to this recommendation, we will provide updated information.
|
| Veterans Health Administration | The Under Secretary for Health should ensure that the annual facility self-assessment and VISN audit includes (1) an assessment of facility adherence to all VHA policy requirements for timeliness and maintenance of required documentation; and (2) a sample of providers who underwent quality reviews and SLB or NPDB reporting. (Recommendation 7) |
When we confirm what actions the agency has taken in response to this recommendation, we will provide updated information.
|