Veterans Choice Program: Improvements Needed to Address Access-Related Challenges as VA Plans Consolidation of its Community Care Programs
Fast Facts
If services are not readily accessible at VA medical facilities, the Veterans Choice Program allows eligible veterans to receive care from non-VA providers. Congress created the temporary program in 2014, aiming to alleviate the excessive wait times some veterans faced at VA.
However, we found that it’s unclear if the Choice Program improved the timeliness of veterans’ care because VA’s data are incomplete and unreliable.
When the Choice Program ends, veterans will still receive care from non-VA providers through a new program. We made recommendations related to improving VA’s ability to monitor veterans’ access to care through the new program.

A photo of a patient getting their blood pressure checked.
Highlights
What GAO Found
Through the Veterans Choice Program (Choice Program), eligible veterans may receive care from community providers when it is not readily accessible at Veterans' Health Administration (VHA) medical facilities. The Department of Veterans Affairs (VA) uses two contractors—or third party administrators (TPA)—to schedule most veterans' Choice Program appointments after receiving referrals from VA medical centers (VAMC). GAO found that veterans who are referred to the Choice Program for routine care because services are not available at VA in a timely manner could potentially wait up to 70 calendar days for care if VAMCs and the TPAs take the maximum amount of time VA allows to complete its appointment scheduling process. This is not consistent with the statutory requirement that veterans receive Choice Program care within 30 days of their clinically indicated date (when available), which is the soonest date that it would be appropriate for the veteran to receive care, according to a VHA clinician. Without designing appointment scheduling processes that are consistent with this requirement, VA lacks assurance that veterans will receive Choice Program care in a timely manner.
GAO and VHA found that selected veterans experienced lengthy actual wait times for appointments in 2016, after manually reviewing separate samples of Choice Program authorizations. For example, when GAO analyzed 55 routine care authorizations that were created between January and April of 2016, it found that the process took at least 64 calendar days, on average. When VHA analyzed about 5,000 authorizations created between July and September of 2016, it took an average of 51 calendar days for veterans to receive care.
Average Wait Times for Choice Program Appointments in 2016, According to Separate Non-Generalizable Analyses by GAO and the Veterans Health Administration (VHA)a
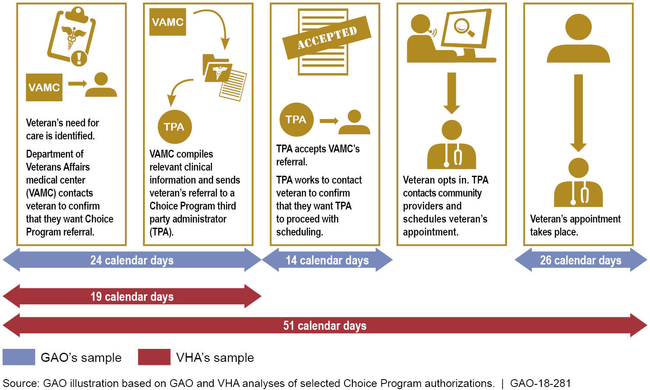
aGAO excluded from its analysis the amount of time the TPA took to schedule the appointment and the overall wait time because its sample selection methodology differed from VHA's in a way that would have skewed these two averages but not the averages for the other segments of the process.
GAO also found that VHA cannot systematically monitor the timeliness of veterans’ access to Choice Program care because it lacks complete, reliable data to do so. The data limitations GAO identified include:
- A lack of data on the timeliness of referring and opting veterans in to the program. GAO found that the data VHA uses to monitor the timeliness of Choice Program appointments do not capture the time it takes VAMCs to prepare veterans’ referrals and send them to the TPAs, nor do they capture the time spent by the TPAs in accepting VAMCs’ referrals and opting veterans in to the Choice Program. VHA has implemented an interim solution to monitor overall wait times that relies on VAMC staff consistently and accurately entering unique identification numbers on VHA clinicians’ requests for care and on Choice Program referrals, a process that is prone to error.
- Inaccuracy of clinically indicated dates. GAO found that clinically indicated dates (which are used to measure the timeliness of care) are sometimes changed by VAMC staff before they send Choice Program referrals to the TPAs, which could mask veterans’ true wait times. GAO found that VAMC staff entered later clinically indicated dates on referrals for about 23 percent of the 196 authorizations it reviewed. It is unclear if VAMC staff mistakenly entered incorrect dates manually, or if they inappropriately entered later dates when the VAMC was delayed in contacting the veteran, compiling relevant clinical information, and sending the referral to the TPA.
- Unreliable data on the timeliness of urgent care. GAO found that VAMCs and TPAs do not always categorize Choice Program referrals and authorizations in accordance with the contractual definition for urgent care. According to the contracts, a referral is to be marked as “urgent,” and an appointment is to take place within 2 days of the TPA accepting it, when a VHA clinician has determined that the needed care is (1) essential to evaluate and stabilize the veteran’s condition, and (2) if delayed would likely result in unacceptable morbidity or pain. GAO reviewed a sample of 53 urgent care authorizations and determined that about 28 percent of the authorizations were originally marked as routine care authorizations but were changed to urgent by VAMC or TPA staff, in an effort to administratively expedite appointment scheduling.
Why GAO Did This Study
Congress created the Choice Program in 2014 to address longstanding challenges with veterans' access to care at VHA medical facilities. The Joint Explanatory Statement for the Consolidated Appropriations Act, 2016 included provisions for GAO to review veterans' access to care through the Choice Program.
This report examines for Choice Program care (1) VA's appointment scheduling process, (2) the timeliness of appointments and the information VHA uses to monitor veterans' access; and (3) the factors that have adversely affected veterans' access and the steps VA and VHA have taken to address them for VA's future community care program.
GAO reviewed applicable laws and regulations, VA's TPA contracts, and relevant VHA policies and guidance. Absent reliable national data, GAO also selected 6 of 170 VAMCs (selected for variation in geographic location and the TPAs that served them) and manually reviewed a random, non-generalizable sample of 196 Choice Program authorizations. The authorizations were created for veterans who were referred to the program between January and April of 2016, the most recent period for which data were available when GAO began its review. The sample of authorizations included 55 for routine care, 53 for urgent care, and 88 that the TPAs returned without scheduling appointments. GAO also obtained the results of VHA's non-generalizable analysis of wait times for a nationwide sample of about 5,000 Choice Program authorizations that were created for selected services between July and September of 2016.
Recommendations
For VA's future consolidated community care program, GAO is making 10 recommendations, which include:
- establishing an achieveable wait-time goal for the community care program that will permit VHA to monitor whether veterans are receiving care within time frames that are comparable to the amout of time they would otherwise wait for care at VHA medical facilities;
- designing an appointment scheduling process that (1) is consistent with the wait-time goal and (2) sets forth time frames within which veterans' referrals must be processed, appointments must be scheduled, and appointments must occur;
-
implementing mechanisms to:
- allow VHA to systematically monitor the amount of time taken to prepare referrals, schedule appointments, and complete appointments;
- prevent veterans' clinically indicated dates from being modified by individuals other than VHA clinicians; and
- separate clinically urgent referrals and authorizations from those for which the VAMC or the TPA has decided to expedite appointment scheduling for administrative reasons; and
- establishing a system that will help facilitate seamless, efficient care coordination and exchanges of information among VAMCs, VHA clinicians, TPAs, community providers, and veterans.
VA generally agreed with all but one of GAO's recommendations, which was to separate clinically urgent referrals from those that are administratively expedited. GAO maintains that implementing this recommendation will help improve future monitoring of urgent care timeliness for reasons explained in the report.
Recommendations for Executive Action
| Agency Affected | Recommendation | Status |
|---|---|---|
| Office of the Under Secretary for Health |
Priority Rec.
The Under Secretary for Health should establish an achievable wait-time goal for the consolidated community care program that VA plans to implement that will permit VHA to monitor whether veterans are receiving VA community care within time frames that are comparable to the amount of time they would otherwise wait to receive care at VHA medical facilities. (Recommendation 1) |
VA agreed with our recommendation. VA officials stated that they use two methods to monitor veterans' access to community care. First, VA has defined some time frames for VA medical center staff to meet when scheduling community care appointments. Second, VA monitors network adequacy standards under the current contracts with community care contractors. However, as of February 2026, VA has not yet defined a timeliness standard for when veterans should receive care under the Veterans Community Care Program. By not addressing this recommendation, VA increases its risk of not being able to ensure that all veterans receive timely access to community care.
|
| Office of the Under Secretary for Health |
Priority Rec.
The Under Secretary for Health should design an appointment scheduling process for the consolidated community care program that VA plans to implement that sets forth time frames within which (1) veterans' referrals must be processed, (2) veterans' appointments must be scheduled, and (3) veterans' appointments must occur, which are consistent with the wait-time goal VHA has established for the program. (Recommendation 2) |
VA agreed with our recommendation and has defined time frames for when a community care referral must be processed and scheduled. As of February 2026, VA has not yet defined a timeliness standard for when a veteran's appointment should occur. Once this standard is established, VA can takes steps to ensure the current scheduling process and time frames for the VCCP allow the department to achieve that standard to help ensure that all veterans receive timely access to community care.
|
| Office of the Under Secretary for Health | The Under Secretary for Health should establish a mechanism that will allow VHA to systematically monitor the average number of days it takes for VAMCs to prepare referrals, for VAMCs or TPAs to schedule veterans' appointments, and for veterans' appointments to occur, under the consolidated community care program that VA plans to implement. (Recommendation 3) |
The Veterans Health Administration (VHA) agreed with our recommendation and in June 2019, VHA implemented its new consolidated community care program-the Veterans Community Care Program (VCCP). In addition, VHA developed and fully deployed the HealthShare Referral Manager (HSRM), a software system for VA medical center staff to use to manage VCCP referrals. In June 2021, VA officials provided a copy of an HSRM referral report that can display the number of days it takes for a VA medical center to prepare a referral, for a veteran's appointment to be scheduled, and for the veteran's appointment to occur. By implementing the HSRM and its reporting capabilities, VHA has taken action to establish a mechanism to monitor time frames in the referral lifecycle.
|
| Office of the Under Secretary for Health | The Under Secretary for Health should implement a mechanism to prevent veterans' clinically indicated dates from being modified by individuals other than VHA clinicians when veterans are referred to the consolidated community care program that VA plans to implement. (Recommendation 4) |
Our report recommended that the Under Secretary for Health implement a mechanism to prevent veterans' clinically indicated dates (CID) from being modified by individuals other than VHA clinicians when veterans are referred to community care. The Veterans Health Administration (VHA) developed the HealthShare Referral Manager (HSRM) for staff to use to manage community care referrals under the Veterans Community Care Program, and deployed the HSRM at all VA medical centers (VAMC) as of June 24, 2019. In March 2020, VHA provided documentation that shows (1) the VHA clinician populates the CID field when they create the referral in VA's electronic medical record system, (2) when the referral is forwarded to HSRM for referral management and appointment scheduling by VAMC staff, the CID field in HSRM is auto-populated based on the CID in VA's electronic medical record system, and (3) the auto-populated CID field in HSRM cannot be edited. In addition, VHA officials stated in April 2021 that only the VA ordering provider or other clinical staff with proper authority can edit a CID, which results in the referral being canceled and re-reviewed by the ordering VA provider. Based on VHA's actions and assurance that appropriate mechanisms are in place to prevent the CID from being inappropriately changed by individuals other than the VA provider or authorized staff, we are closing this recommendation.
|
| Office of the Under Secretary for Health | The Under Secretary for Health should implement a mechanism to separate clinically urgent referrals and authorizations from those for which the VAMC or the TPA has decided to expedite appointment scheduling for administrative reasons. (Recommendation 5) |
In June 2021, Veterans Health Administration (VHA) officials stated that VHA's new community provider network contracts and IT systems do not allow for any VA or contractor staff to change the urgency of a referral after the determination of urgency has been made by the ordering VA provider. VHA officials stated that the status of the referral can only be altered by the ordering VA provider if the referral is canceled and resubmitted. Due to the changes made by VHA under its new contracts for the Veterans Community Care Program, and assurances that only the ordering VA provider can alter the status of a referral, we consider this recommendation implemented.
|
| Office of the Under Secretary for Health | The Under Secretary for Health should (1) establish oversight mechanisms to ensure that VHA is collecting reliable data on the reasons that VAMC or TPA staff are unsuccessful in scheduling veterans' appointments through the consolidated community care program VA plans to implement, and (2) demonstrate that it has corrected any identified deficiencies. (Recommendation 6) |
The Veterans Health Administration (VHA) agreed with our recommendation and stated in January 2021 that it had established an oversight mechanism to track VA staff scheduling contact attempts for community care referrals, and has created oversight reports to monitor scheduling challenges. In May 2021, VHA confirmed that the third-party administrators (TPA), when scheduling veteran appointments, are to return referrals back to VA if they encounter scheduling problems within 10 days. In addition, TPA staff are also to select a code for each referral as to why they were unable to schedule an appointment. VHA officials stated that they create reports based on TPA scheduling challenges, and review those reports on a monthly basis. Based on VHA's actions, we are closing this recommendation.
|
| Department of Veterans Affairs | The Secretary of Veterans Affairs should ensure that the contracts for the consolidated community care program VA plans to implement include performance metrics that will allow VHA to monitor average driving times between veterans' homes and the practice locations of community providers that participate in the TPAs' networks. (Recommendation 7) |
The Veterans Health Administration (VHA) agreed with this recommendation, and as of February 2021, reported that it included performance metrics related to drive times in its contracts for the new third-party administrators in Regions 1-5 of the new Community Care Network (CCN) under the Veterans Community Care Program. VHA officials stated that the agency plans for the last contract to include the same metrics to be consistent throughout the CCN. Based on VHA's actions, we are closing this recommendation.
|
| Department of Veterans Affairs |
Priority Rec.
The Secretary of Veterans Affairs should establish a system for the consolidated community care program VA plans to implement to help facilitate seamless, efficient information sharing among VAMCs, VHA clinicians, TPAs, community providers, and veterans. Specifically, this system should allow all of these entities to electronically exchange information for the purposes of care coordination. (Recommendation 8) |
Our report recommended that the Under Secretary for Health should establish a system for the consolidated community care program the Veterans Health Administration (VHA) plans to implement to help facilitate seamless, efficient information sharing among VA medical centers (VAMC), VHA clinicians, third-party administrators, community providers, and veterans that would allow all of these entities to electronically exchange information for the purposes of care coordination. In June 2019, VHA implemented its new consolidated community care program-the Veterans Community Care Program (VCCP). In addition, VHA developed the HealthShare Referral Manager (HSRM), a software system for VAMC staff to use to manage VCCP referrals, including creating authorizations, scheduling veteran appointments, and exchanging documentation electronically with community providers. VHA deployed the HSRM at all VAMCs as of June 24, 2019, and according to VHA officials, the system was fully implemented as of December 31, 2019. In addition, in March 2020, VHA officials stated veterans are able to use VA Online Scheduling, which is a mobile scheduling application for veterans to request community care appointments and document scheduling preferences, and My HealtheVet, which is a website where veterans can refill prescriptions, review appointments, send electronic messages to VHA staff, and view their medical records. By implementing the HSRM and options for veterans to electronically interact with VHA staff, VHA has taken action to facilitate information sharing among various entities for the purposes of care coordination.
|
| Office of the Under Secretary for Health | The Under Secretary for Health should conduct a comprehensive evaluation of the outcomes of the two appointment scheduling pilots it established at the Alaska and Fargo VA Health Care Systems (where VAMC staff, rather than TPA staff, are responsible for scheduling veterans' Choice Program appointments), which should include a comparison of the timeliness with which VAMC staff and TPA staff completed each step of the Choice Program appointment scheduling process, as well as the overall timeliness with which veterans received appointments. (Recommendation 9) |
In July 2016 and October 2016, the Veterans Health Administration (VHA) began pilot projects at two VA medical centers (VAMC) where VAMC staff took over scheduling Choice Program appointments from the third-party administrators (TPA). We recommended in our 2018 report that VHA evaluate the outcome of those two pilots-specifically, comparing the timeliness of VAMC staff scheduling Choice Program appointments against TPA's scheduling Choice Program appointments-to inform its planning and decisions for VAMC staff scheduling under its planned consolidated community care program, and identify any risks to VAMC staff scheduling under the new program. In June 2019, VA implemented its new consolidated community care program-the Veterans Community Care Program (VCCP). In November 2018, VHA officials stated that after reviewing the data from the pilots, VHA was unable to determine the timeliness of VAMC staff appointment scheduling due to the manual processes involved in appointment scheduling. In July 2019, VHA again stated that it was unable to conduct the comprehensive evaluation of the pilots, but that it planned to use the HealthShare Referral Manager (HSRM), once implemented, to track the timeliness of appointment scheduling by VAMC staff under the VCCP. Our recommendation was intended for VHA to compare the timeliness of appointment scheduling by VAMC staff and TPA staff under the Choice Program, which expired over a year ago, to inform VHA's planning and implementation of appointment scheduling responsibilities under the VCCP. VHA was (1) unable to complete the evaluation, and (2) VHA's recent updates of using the HSRM to track timeliness of current VAMC staff appointment scheduling are not relevant to the intent of our recommendation. Therefore, we have closed this recommendation as not implemented based on these reasons.
|
| Office of the Under Secretary for Health | The Under Secretary for Health should issue a comprehensive policy directive and operations manual for the consolidated community care program VA plans to implement and ensure that these documents are reviewed and updated in a timely manner after any significant changes to the program occur. (Recommendation 10) |
The Veterans Health Administration (VHA) agreed in principle with this recommendation, and in April 2026, officials stated that the planned policy directive is still in the concurrence process. VHA officials anticipate publishing the directive in July 2026.
|