Veteran Suicide: VA Needs Accurate Data and Comprehensive Analyses to Better Understand On-Campus Suicides
Fast Facts
Preventing veteran suicide is the Department of Veterans Affairs' highest clinical priority. The VA started tracking suicide deaths on VA campuses—medical facilities, parking areas, and cemeteries—in October 2017 and identified 55 on-campus veteran suicides through September 2019.
We reviewed the VA's data and found errors: 4 missing cases that should've been counted and 10 cases that shouldn't have been—including a veteran who was alive. Also, the VA isn't fully using data it already has to analyze these suicides.
We recommended that the VA improve how it tracks and analyzes this data to better address and prevent on-campus veteran suicides.
Heightened barriers at a VA medical facility parking garage to prevent efforts to jump off of the structure

Highlights
What GAO Found
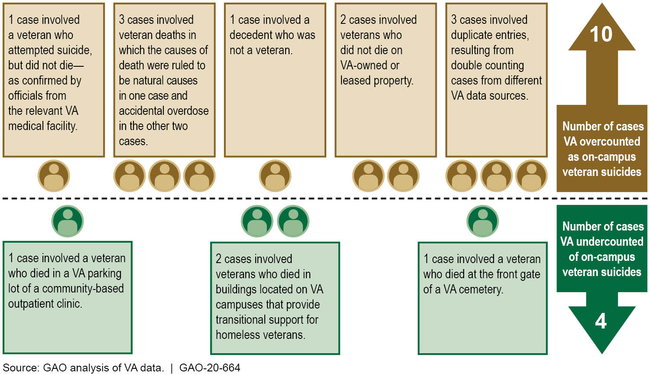
The Department of Veterans Affairs' (VA) process for identifying on-campus suicides does not include a step for ensuring the accuracy of the number of suicides identified. As a result, its numbers are inaccurate. VA's Veterans Health Administration (VHA) first started tracking on-campus veteran suicides in October 2017, and uses the results to inform VA leadership and Congress. GAO reviewed the data and found errors in the 55 on-campus veteran suicides VHA identified for fiscal years 2018 and 2019, including 10 overcounts (deaths that should not have been reported but were) and four undercounts (deaths that should have been reported but were not).
Examples of Errors on the Department of Veterans Affairs' (VA) List of 55 On-Campus Veteran Suicides for Fiscal Years 2018 and 2019 (as of September 2019)
VA has taken some steps to address on-campus veteran suicides, such as issuing guidance and staff training. However, GAO found that the analyses informing these efforts are limited. Specifically, VHA
- requires root cause analyses—processes to determine what can be done to prevent recurrences of incidents—for some but not all on-campus veteran suicides. According to VHA officials, only 25 percent of on-campus suicides from October 2017 to April 2019 met the criteria for a root cause analysis.
- does not make use of all relevant information VA collects about these deaths, such as clinical and demographic data collected through other VA suicide prevention efforts. VHA officials said they could not link the different sources of information, but GAO found that selected medical facilities could do so.
Without accurate information on the number of suicides and comprehensive analyses of the underlying causes, VA does not have a full understanding of the prevalence and nature of on-campus suicides, hindering its ability to address them.
Why GAO Did This Study
VA established suicide prevention as its highest clinical priority. In recent years, there have been reports of veterans dying by suicide on VA campuses—in locations such as inpatient settings, parking lots, and on the grounds of cemeteries.
GAO was asked to review veteran deaths by suicide on VA campuses. This report examines (1) VA's process to track the number of veterans that died by suicide on VA campuses, and (2) steps VA has taken to address these types of suicides.
GAO reviewed the sources of information VHA uses to identify and analyze on-campus veteran suicides, VA and VHA strategic plans and policies related to suicide prevention and reporting, and federal internal control standards. GAO also interviewed VA and VHA central office officials, and officials from three medical facilities that GAO selected because they reportedly had on-campus veteran suicides between fiscal years 2018 and 2019.
Recommendations
GAO is making three recommendations, including that VA improve its process to accurately identify all on-campus veteran suicides and conduct more comprehensive analyses of these occurrences. VA did not concur with one of GAO's recommendations related to conducting root cause analyses. GAO continues to believe that this recommendation is valid, as discussed in the report.
Recommendations for Executive Action
| Agency Affected | Recommendation | Status |
|---|---|---|
| Department of Veterans Affairs |
Priority Rec.
The Under Secretary for Health should, in collaboration with relevant VBA and NCA officials, improve its process to accurately identify all on-campus veteran deaths by suicide by ensuring that it uses updated information and corroborates information with VA facility officials. (Recommendation 1) |
On September 16, 2022, VA published VA-wide reporting procedures for suicide deaths on VA property-which the procedures define as any VA owned, rented, or leased property where the VA has physical possession and under the purview of VA's Office of Operations, Security, and Preparedness. The procedures direct each VA administration to maintain data on suicide deaths and to provide information to the Office of Mental Health and Suicide Prevention for reconciliation and analysis.
|
| Department of Veterans Affairs |
Priority Rec.
The Under Secretary for Health should expand the policy requirement for a root cause analysis to include all cases of on-campus veteran death by suicide, regardless of whether the veterans involved were enrolled in VHA health care services at the time of their death. (Recommendation 2) |
VA disagreed with our recommendation and stated that a root cause analysis was not the appropriate tool for conducting suicide surveillance for all cases of veteran death by suicide. However, VA did agree with the importance to capture data and study individual deaths by suicide on VA property in order to be able to identify trends to improve VA actions. In January 2022, VA stated that VHA requires facilities to submit Issue Briefs for all suicide attempts and deaths that occur at VA medical centers. In August 2022, VHA released guidance to VA organizations that expanded its data collection processes for Issue Briefs when deaths by suicide occur on VA property. The updated Issue Brief format directs VA medical centers to include a statement confirming that a root cause analysis will be completed or, in cases where a root cause analysis is optional, why the root cause analysis will not be completed. VA also completed a report in July 2022 entitled On-Campus Suicide Deaths Among Veterans: Detailed Analyses of Data from Issue Briefs, Chart Reviews, and Root Causes Analyses. The report identified areas for improvement based on the 29 on-campus suicide deaths that occurred in fiscal years 2020 and 2021. Because VA has taken steps to improve data collection on individual deaths by suicide through its Issue Brief process and is using information to study the issue of on-campus suicides, VA has fulfilled the intent of our recommendation.
|
| Department of Veterans Affairs | The Under Secretary for Health should direct the Office of Mental Health and Suicide Prevention to expand its analyses of on-campus veteran deaths by suicide to include all relevant information VA collects for these incidents, such as data from root causes analyses and information collected through the Behavioral Health Autopsy Program. (Recommendation 3) |
VA concurred with this recommendation. In July 2022, VA completed a report entitled On-Campus Suicide Deaths Among Veterans: Detailed Analyses of Data from Issue Briefs, Chart Reviews, and Root Causes Analyses. The report identified areas for improvement based on the 29 on-campus suicide deaths that occurred in fiscal years 2020 and 2021, and included information from Issue Briefs, Root Causes Analyses, and information from Behavioral Health Autopsy Chart Reviews. VA's report also acknowledged that collecting comprehensive details about on-campus suicides is essential to create a better, safer environment of care for veterans, and that key VA stakeholders will convene to draft recommendations for VA leadership, Veterans Integrated Services Networks and VA facilities to assist with efforts to reduce Veteran suicide on VA property.
|