Telehealth: Use in Medicare and Medicaid
Fast Facts
Do Medicare and Medicaid pay when beneficiaries use two-way video visits to get care from their doctors?
It depends. Medicare pays for some two-way video visits—referred to as "telehealth"—if the patients connect from rural health facilities. Medicare is testing new ways to provide health care that allow telehealth coverage regardless of location.
Under Medicaid, states may cover different types of telehealth services from different types of care providers.
In the 6 states we reviewed, officials from states that were generally more rural said they used telehealth more frequently than officials from more urban states.
Example of Telehealth Use with Medicare
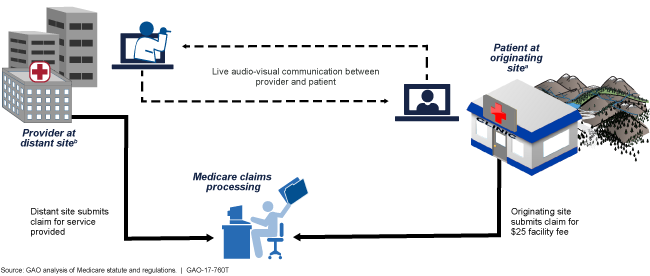
Illustrated flow chart of a telehealth session and how Medicare handles the related claims.
Highlights
What GAO Found
Available analysis GAO reviewed shows that Medicare providers used telehealth services (providing clinical care remotely by 2-way video) for a small proportion of beneficiaries and relatively few services in calendar year 2014. Specifically, an analysis of Medicare claims data by the Medicare Payment Advisory Commission shows that about 68,000 Medicare beneficiaries—0.2 percent of Medicare Part B fee-for-service beneficiaries—accessed services using telehealth. The most common telehealth visits in calendar year 2014 were for evaluation and management services (66 percent), followed by psychiatric visits (19 percent). In Medicaid, the use of telehealth varies by state. Individual states have the option to determine whether to cover telehealth, what types of telehealth services to cover, and which types of providers can receive reimbursement for telehealth services, among other things. In the six states GAO reviewed, officials from states that were generally more rural than urban said they used telehealth more frequently than officials from more urban states.
Selected provider, patient, and payer associations GAO interviewed reported that telehealth may improve care for Medicare beneficiaries, but they also cited coverage and payment restrictions as barriers to the use of telehealth in Medicare.
Officials from the selected associations reported several factors that encourage the use of telehealth in Medicare, including the potential to improve or maintain quality of care in Medicare, alleviate provider shortages, and increase convenience to patients. For example, officials from one provider association noted that provider and regional medical specialty shortages can be addressed through telehealth, potentially increasing productivity and ensuring on-time scheduling of appointments.
Officials from the selected associations also reported several potential barriers to the use of telehealth in Medicare, including payment, coverage restrictions, and infrastructure requirements. For example, officials from one provider association and both of the selected patient associations described access to sufficiently reliable broadband internet service as a barrier to telehealth use.
The Centers for Medicare & Medicaid Services (CMS), which administers Medicare, has various efforts underway that have the potential to expand the use of telehealth in Medicare. As of April 2017, CMS was supporting eight such models and demonstrations. For example, CMS's Frontier Community Health Integration Project Demonstration aims to develop and test new models of integrated health care in sparsely populated rural counties. Under the demonstration, CMS allows participating providers to receive cost-based payments for telehealth when their location serves as the originating site, rather than the approximately $25 fixed fee that CMS otherwise pays originating sites.
Why GAO Did This Study
Telehealth can provide an alternative to health care provided in person at a physician's office, particularly for patients who cannot easily travel long distances for care. Medicare pays for some telehealth services that are subject to statutory and regulatory requirements, such as requiring the patient be present at an originating site like a rural health clinic.
This testimony discusses (1) the extent to which telehealth is used by Medicare and Medicaid to provide health care services; (2) factors selected associations representing providers, patients, and payers reported as affecting the use of telehealth in Medicare; and (3) how emerging payment and delivery models could affect the potential use of telehealth in Medicare.
This testimony is based on GAO's April 2017 report ( GAO-17-365 ). For that report, GAO reviewed agency documents and regulations and interviewed Medicare agency officials and Medicaid officials from six states, selected based on multiple factors, including rural population. GAO also selected specialty associations with expertise and interest in telehealth—five provider, two patient, and one payer association—based on a review of documents and literature and through background interviews. GAO interviewed representatives from each of the associations and also collected information from the provider and patient associations through a data collection instrument. In addition, GAO reviewed agency documents describing and evaluating the models and demonstrations that support alternative approaches to health care payment and delivery.
For more information, contact A. Nicole Clowers at (202) 512-7114 or clowersa@gao.gov.