Hospital Value-Based Purchasing: CMS Should Take Steps to Ensure Lower Quality Hospitals Do Not Qualify for Bonuses
Fast Facts
Through the Hospital Value-based Purchasing program, hospitals that participate in Medicare receive bonuses or penalties, depending on their performance on a set of quality and efficiency measures.
Despite the program's intention to reward hospitals that provide high-quality care at a lower cost, we found that some hospitals with low quality scores received bonuses because they had relatively high efficiency scores.
To ensure that lower quality hospitals do not receive these bonuses, we recommended that the Centers for Medicare & Medicaid Services revise the methodology this program uses to calculate total performance scores.
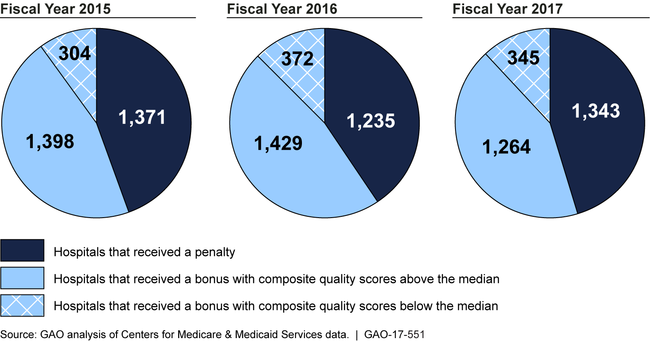
Bonus or Penalty Status of Hospitals Participating in the Hospital Value-based Purchasing Program, Fiscal Years 2015-2017
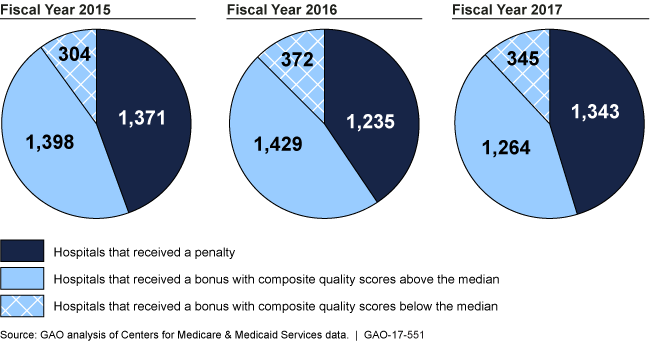
Number of participating hospitals that received bonuses or penalties.
Highlights
What GAO Found
The Hospital Value-based Purchasing (HVBP) program aims to improve quality of care and efficiency by creating financial incentives for about 3,000 participating hospitals. From fiscal years 2013 through 2017, performance on quality and efficiency measures varied by hospital type. Safety net hospitals—those that serve a high proportion of low-income patients—generally scored lower in quality compared to all participating hospitals. In contrast, small rural and small urban hospitals—those with 100 or fewer acute care beds—scored higher on efficiency compared to all hospitals.
Payment adjustments—bonuses or penalties, announced prior to each fiscal year—have varied over time for all hospitals. In four out of the five years of GAO's analysis, small rural and small urban hospitals were more likely to receive a bonus compared to all participating hospitals, while safety net hospitals were more likely to receive a penalty. While a majority of all hospitals received a bonus or a penalty of less than 0.5 percent each year, the percentage of hospitals receiving a bonus greater than 0.5 percent increased from 4 percent to 29 percent from fiscal year 2013 to 2017. In dollar terms, most hospitals had a bonus or penalty of less than $100,000 in fiscal year 2017.
Some hospitals with high efficiency scores received bonuses, despite having relatively low quality scores, which contradicts the Centers for Medicare & Medicaid Service's (CMS) stated intention to reward hospitals providing high-quality care at a lower cost. Further, among hospitals that were missing one or more quality scores, the efficiency score had a greater effect on the total performance score because of the methodology used by CMS. This methodology compensated for the missing scores by increasing the weights of all of the non-missing scores. Consequently, hospitals with missing scores were more likely to receive bonuses than hospitals with complete scores.
Bonus or Penalty Status of Hospitals Participating in the Hospital Value-based Purchasing Program, Fiscal Years 2015 through 2017
Why GAO Did This Study
The HVBP program, enacted as part of the Patient Protection and Affordable Care Act (PPACA), evaluates hospital performance on quality and efficiency (Medicare spending per beneficiary) measures. Based on those results, CMS adjusts Medicare payments, leading to bonuses or penalties for hospitals. The first HVBP payment adjustments started in fiscal year 2013.
PPACA included a provision for GAO to assess the HVBP program's impact on Medicare quality and efficiency, including the effects on safety net, small rural, and small urban hospitals. This report addresses (1) hospitals' performance in quality and efficiency categories; (2) how hospitals' payment adjustments have changed over time; and (3) the effect, if any, of efficiency scores on payment adjustments.
GAO analyzed CMS documentation and data on performance scores and payment adjustments in each year for all hospitals participating in fiscal years 2013 through 2017. GAO also analyzed results for safety net, small rural, and small urban hospitals and interviewed CMS officials.
Recommendations
So that lower quality hospitals do not receive bonuses, GAO recommends that CMS revise (1) the methodology used to calculate total performance scores and (2) its method of accounting for missing quality scores. In its written comments, HHS indicated that it would consider revising these two methodologies.
Recommendations for Executive Action
| Agency Affected | Recommendation | Status |
|---|---|---|
| Centers for Medicare & Medicaid Services | To ensure that the HVBP program accomplishes its goal to balance quality and efficiency and to ensure that it minimizes the payment of bonuses to hospitals with lower quality scores, the Administrator of CMS should revise the formula for the calculation of hospitals' total performance score or take other actions so that the efficiency score does not have a disproportionate effect on the total performance score. |
CMS has taken actions to address our recommendation. Starting in 2018, CMS began examining ways to revise the formula for the calculation of hospitals' total performance scores (TPS) to reduce the effect of the efficiency domain on the TPS. In 2019 CMS proposed removing the safety domain and increasing the weight of the clinical care domain, which was estimated to reduce the effect of the efficiency domain on the TPS. However, stakeholders raised concerns about the adverse impacts to rural and smaller hospitals from such a change. CMS indicated that its analysis confirmed this trend, and the agency therefore decided not the change the measure weights. In January 2023, CMS provided documentation demonstrating that it had revised, tested, and adopted a measure in the efficiency domain. In August 2023, CMS issued a final rule in which it implemented the revision in its hospital Inpatient Quality Reporting (IQR) program. CMS stated that the revision would be moved into to the HVBP Program once the statutory requirement of being first publicly reported for a year in the Hospital IQR program had been met. With the revised measure, CMS will achieve greater balance between quality and efficiency in the HVBP program and minimize bonus payments to lower quality hospitals.
|
| Centers for Medicare & Medicaid Services | To ensure that the HVBP program accomplishes its goal to balance quality and efficiency and to ensure that it minimizes the payment of bonuses to hospitals with lower quality scores, the Administrator of CMS should revise the practice of proportional redistribution used to correct for missing domain scores so that it no longer facilitates the awarding of bonuses to hospitals with lower quality scores. |
CMS indicated that it would explore alternatives to the practice of proportional redistribution, and any changes to the distribution of weights for missing domains would be evaluated for potential negative impacts and would be subject to notice and comment rulemaking. Although CMS did not directly revise the practice of proportional redistribution, the agency took other actions that mitigate the effects of this practice, particularly the awarding of bonuses to lower-quality hospitals. For example, CMS indicated that in fiscal year 2017, hospitals would be required to receive scores in at least three, instead of two domains, thus reducing the effect of proportional redistribution for missing domain scores. Further, in August 2023, CMS issued a final rule in which the agency included a new measure to the safety domain related to the management of patients with severe sepsis shock. CMS indicated that the addition of this measure supports the efficient and timely delivery of high-quality sepsis care and may allow more hospitals to receive a score in the safety domain, thereby reducing the number of hospitals with missing scores in the domain. CMS also finalized a scoring methodology change that gives hospitals the opportunity to receive up to ten points toward their Total Performance Score based on the proportion of patients treated that are dually eligible and the hospital's performance on existing HVBP measures. According to CMS, the scoring methodology update was purposefully designed not to reward poor quality, but to give the highest rewards to hospitals caring for a larger proportion of underserved patients and delivering high quality care to all populations they serve. Thus, these scoring changes will likely help minimize bonus payments to hospitals with lower quality scores.
|