Medicaid: States Fund Services for Adults in Institutions for Mental Disease Using a Variety of Strategies
Fast Facts
Federal and state Medicaid spending on behavioral health services—mental health and substance use treatments—is projected to be $71 billion in 2017.
However, some adults on Medicaid may have limited access to inpatient or residential behavioral health care because Medicaid generally doesn't cover services for adults in institutions for mental disease.
Officials in the 6 states we reviewed tried an average of 2 to 4 strategies to fund this care through Medicaid, such as
Applying for demonstration programs
Covering these services through Medicaid managed care plans
Relying on facilities that are too small to be considered "institutions"
Percentage of Adults with Serious Mental Health Conditions, Substance Use Conditions, or Co-occurring Serious Mental Health and Substance Use Conditions, by Insurance Status, 2015
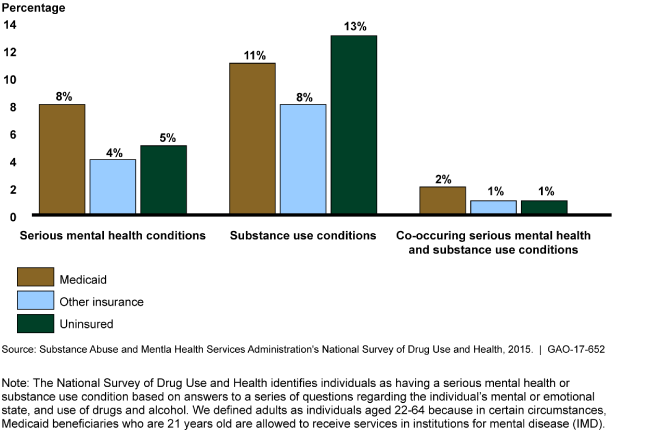
Adults enrolled in Medicaid had higher rates of serious mental health conditions than other groups.
Highlights
What GAO Found
Between 2010 and 2015, inpatient and residential behavioral health services capacity has gone up for adult mental health treatment and stayed about the same for substance use treatment. GAO found that for adult mental health treatment, inpatient and residential capacity increased from about 61 to 69 beds per 100,000 adults between 2010 and 2014. For adult substance use treatment, inpatient and residential capacity remained fairly constant between 2010 and 2015, increasing from 57 to about 58 beds per 100,000 adults. In both types of behavioral health services there was significant variation across states.
GAO also found that over time, the Centers for Medicare & Medicaid Services' (CMS)—the agency that oversees state Medicaid programs—changed policies to allow some states to finance care for adult Medicaid beneficiaries in institutions for mental disease (IMD), in certain circumstances. IMDs are generally facilities larger than 16 beds that primarily provide inpatient, residential, or other services to individuals with behavioral health conditions. These policy changes included the following:
Medicaid demonstrations. Beginning in 1993, CMS officials said they approved demonstrations in nine states, allowing federal funds to cover behavioral health services in IMDs; these demonstrations were largely phased out by 2009. In July 2015, CMS announced a demonstration that would allow states to use Medicaid funds to cover substance use services in IMDs. As of May 2017, CMS had approved these demonstrations in four states. CMS has also approved applications from some, but not all, states for demonstrations that allow states to pay for substance use or mental health services in IMDs.
Medicaid managed care. In May 2016, CMS issued a final rule that codified a policy, known as the “in lieu of” policy, under which managed care plans may provide alternative services or services in alternative settings, such as IMDs, under certain circumstances. In the rule, CMS set a 15-day per month limit on the number of days an adult beneficiary may receive behavioral health services in an IMD for which managed care plans will receive payment. According to CMS estimates, at least 17 states had likely been allowing such coverage before the rule was issued.
Even with multiple funding sources, selected states reported some problems with adult access to IMD services. While CMS does not collect national data on how states finance services for adults in IMDs, officials in six selected states GAO interviewed stated they used between two to four strategies to fund services for adults in IMDs in recent years, including under Medicaid managed care and demonstrations. State officials said that when their states were unable to use Medicaid funds to finance IMD services, they relied on other options, such as state-only funding, or providing services in smaller non-IMD facilities. Officials from each of the six states shared examples of access problems; for instance, one state reported long waits for inpatient mental health services. In addition, some facility officials said they regularly turned away patients and maintained waitlists.
Why GAO Did This Study
Medicaid is the largest source of national funding for behavioral health services—mental health and substance use services—with nearly $71 billion in projected 2017 spending. However, Medicaid excludes payments for beneficiaries aged 21-64 who are residents of IMDs. As a result, questions have been raised about adult Medicaid beneficiaries' access to services typically provided in IMDs—namely inpatient or residential behavioral health treatments.
GAO was asked to examine questions related to any potential effects of the IMD exclusion on adult beneficiaries. Among other things, this report describes (1) recent trends in the capacity of facilities that provide inpatient and residential behavioral health services; (2) how CMS policies related to the IMD exclusion have changed over time; and (3) how selected states finance IMD services for adult Medicaid beneficiaries. GAO examined federal laws, regulations, and guidance, interviewed officials in the Department of Health and Human Services (HHS), the department that includes CMS, and analyzed the most current data from three national HHS surveys. GAO also interviewed Medicaid officials in six states selected based on geography and use of options to provide care in IMDs for adult Medicaid beneficiaries. Additionally, GAO interviewed representatives of nine behavioral health facilities in the six states referred to GAO by state Medicaid officials and a hospital association. Selected states' and facilities' experiences are not generalizable. HHS provided technical comments on a draft of this report, which GAO incorporated as appropriate.
For more information, contact Katherine Iritani at (202) 512-7114 or iritanik@gao.gov.