Medicaid Managed Care: Improved Oversight Needed of Payment Rates for Long-Term Services and Supports
Fast Facts
Medicaid provides long-term care to states' most vulnerable populations, such as the elderly or disabled. On average, community-based care costs less than at a nursing facility or other institution—and many people prefer it.
States are increasingly paying for long-term care through managed care programs, paying based on set, monthly rates. How states structure these rates—aligning incentives to minimize cost and maximize service—is critical to enhancing community-based care.
On the federal side, we recommended better oversight of the data used to set payment rates, as well as the rates' effect on care and other outcomes.
Illustration of Financial Incentives in a Blended Rate for a Managed Care Organization (MCO) to Provide Community-Based Care
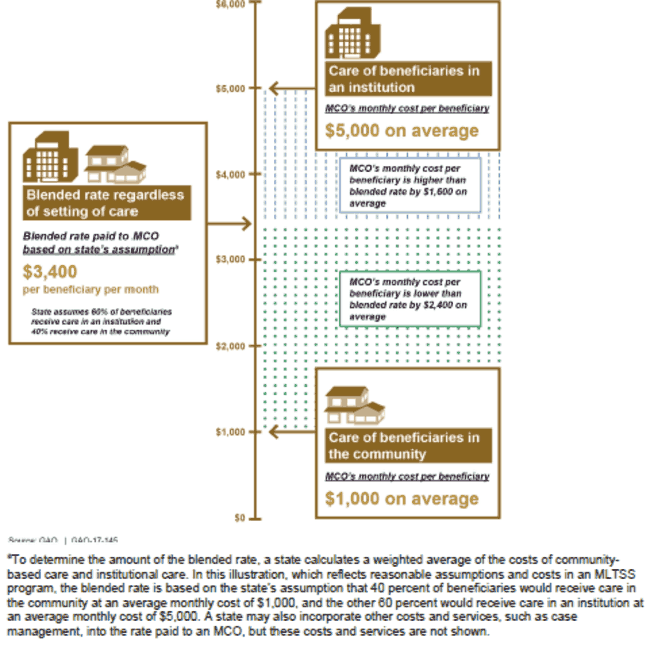
Graphic showing how states may set rates to encourage community-based care.
Highlights
What GAO Found
Out of six states with Medicaid managed long-term services and supports (MLTSS) programs that GAO selected for review, five set clear financial incentives in their payment rates for managed care organizations (MCO) to provide care in the community versus in an institution. However, most of the selected states did not opt to link payments or penalties to MCO performance on MLTSS goals. These goals, which include enhancing the provision of community-based care, are developed by states and the Centers for Medicare & Medicaid Services (CMS), the agency in the Department of Health and Human Services (HHS) responsible for overseeing Medicaid.
GAO found that CMS's oversight of state payment structures was limited. CMS expects states' MLTSS programs to enhance the provision of community-based care. However, GAO found CMS does not consistently require states to report on whether the payment structures—including payment rates, incentive payments, and penalties—are achieving MLTSS goals. For example, CMS required three of the selected states to report on the provision of community-based care, but did not require any such reporting from the other three states. According to federal internal control standards, federal agencies should use quality information to achieve agency objectives. Without requiring information on states' progress toward MLTSS goals, CMS will continue to pay billions of dollars to states without knowing if states have sufficient incentives for community-based care.
In addition, GAO identified risks with CMS's oversight of the data used to set MLTSS rates, specifically the appropriateness and reliability of those data. Under federal regulations, MLTSS rates must be appropriate and adequate. To the extent that states use data that are not appropriate and reliable to set rates, the resulting rates could be too low, which could provide an incentive for MCOs to reduce care, or too high, which results in more federal spending than necessary.
- Appropriateness concerns: GAO found issues with the appropriateness of data used by two of the selected states. For example, one state used data from 2010 and 2011 to set rates for 2015. Beginning in July 2017, CMS will require rates to be based on the three most recent and complete years of data. Although CMS will allow exceptions, it has not specified criteria for what situations would warrant exceptions. Without specifying criteria, CMS's requirements may not sufficiently minimize the number of states using data of questionable appropriateness to set MLTSS rates.
- Reliability concerns: GAO and the HHS Office of Inspector General previously found evidence of reliability issues with managed care encounter data, which are the primary record of managed care services and a key source of data used to set MLTSS rates. In addition, GAO's review of state documentation indicated variation in selected states' procedures for validating the reliability of their encounter data, specifically the completeness and accuracy of the data. Beginning in July 2017, CMS will require states to validate encounter data, but CMS has not issued guidance with minimum standards for state procedures. Without minimum standards for state validation efforts, it is unclear that CMS's efforts will sufficiently minimize the risk of encounter data being incomplete or inaccurate .
Why GAO Did This Study
The provision of long-term services and supports in Medicaid is a significant challenge, because of the vulnerability and service needs of beneficiaries, as well as the high cost of care. An increasing number of states have MLTSS programs, which can be used to expand community-based care and lower costs. However, whether these programs are an effective strategy depends, in part, on the design of the payment structures.
GAO was asked to review states' MLTSS payment structures and CMS's oversight. This report examines (1) how selected states structured their financial incentives, and (2) CMS policies and procedures for overseeing states' payment structures.
GAO reviewed relevant federal regulations, guidance, and internal control standards. For six states selected for variation in location and experience (AZ, DE, FL, KS, MN, and TX), GAO reviewed the contracts and rate certifications most recently approved by CMS, the terms and conditions set by CMS for the programs, and other payment documentation. GAO also interviewed CMS officials and Medicaid officials from the selected states.
Recommendations
GAO recommends CMS (1) require all states to report on progress toward achieving MLTSS program goals, (2) establish criteria for what situations would warrant exceptions to federal standards for data used to set rates, and (3) provide guidance with minimum standards for validating encounter data. HHS concurred with GAO's recommendations.
Recommendations for Executive Action
| Agency Affected | Recommendation | Status |
|---|---|---|
| Centers for Medicare & Medicaid Services | To improve oversight of states' payment structures for MLTSS, the Administrator of CMS should require all states to collect and report on progress toward achieving MLTSS program goals, such as whether the program enhances the provision of community-based care. |
In June 2021, CMS issued guidance to states that triggered the requirement for states to submit annual reports on their Medicaid managed care programs, including MLTSS programs. The guidance indicates that the state annual reports include information on plan performance in providing LTSS. Specifically, the states are to list the performance measures used to assess performance in that area and performance data by plan on those measures. CMS also issued a toolkit in June 2021 for states on developing required managed care quality strategies. This guidance indicates that the strategy include goals and objectives and related performance measures, including around enhancing the provision of community-based LTSS. CMS officials told us that they expect that the measures in state quality strategies will be included in the annual reports. The combination of the guidance on annual reporting and the quality strategy toolkit should result in state reporting that provides CMS with more consistent and comprehensive information on states' progress in meeting MLTSS program goals.
|
| Centers for Medicare & Medicaid Services | To improve oversight of states' payment structures for MLTSS, the Administrator of CMS should establish criteria for what situations would warrant exceptions to the federal standards that the data used to set rates be no older than the three most recent and complete years. |
As of September 2020, CMS reported that it has monitored rate certifications and the data used for rating periods starting on or after July 1, 2017. After three years of monitoring, CMS said that it has not had any states set rates that do not meet the federal standards for the data being no older than the three most recent and complete years, and no states have requested an exception to those standards. The requirements to detail the data being used and the need to explicitly request approval for any exceptions is clearly articulated in annual CMS guidance on rate development. Review of rate certifications in Arizona, a state that had previously used data older than the three most recent and complete years, indicate that the state was meeting the standards and clearly documented that the state was not requesting an exception.
|
| Centers for Medicare & Medicaid Services | To improve oversight of states' payment structures for MLTSS, the Administrator of CMS should provide states with guidance that includes minimum standards for encounter data validation procedures. |
CMS issued an updated state toolkit for validating Medicaid managed care encounter data in December 2019. This toolkit provides information on steps for states to take to validate and improve the Medicaid encounter data they receive from managed care plans. Among other things, the toolkit outlines specific techniques states could use to validate encounter data, including validating specific data fields related to ratesetting. The toolkit categorizes the techniques into four tiers-each of which involves an increasing level of complexity and sources of data-and encourages states to incorporate techniques from all four tiers. In 2022 CMS implemented the transformed Medicaid statistical information system's (T-MSIS) data quality progress for Outcomes Based Data Assessment (OBA). CMS uses the T-MSIS OBA to evaluate state data quality performance under CMS's data quality expectations and work with states to resolve data quality issues identified. Through this process, CMS has identified over 800 issues deemed high priority with state encounter data. In September 2025, CMS provided us information on the OBA that showed that 85 percent of the high priority issues had been resolved as of November 2024. CMS's ongoing assessment of data quality and demonstrated progress working with states to resolve issues combined with guidance provided in the toolkit issued in 2019 addresses GAO's recommendation.
|